

- AI implementation in healthcare means embedding AI into live clinical workflows that handle PHI safely, not picking a model in a demo.
- The first two questions are always the data layer and the legacy core; around 47% of leaders cite data quality as their top barrier.
- Start narrow: diagnostic triage and ambient documentation return clinician time fast, while open-ended ‘vectorize the wiki’ RAG projects fail.
- Clear Minimum Viable Compliance (BAA, HIPAA-eligibility, encryption at creation) before moving a single byte of PHI; eligibility is not compliance.
- Roll out in phases using the Strangler Fig pattern, secure agentic AI against the Lethal Trifecta, and stabilize shaky systems before scaling.
- Done right, AI returns clinician hours and faster diagnoses; done wrong, it leaks six figures in unmonitored token spend.
Q1: What does AI implementation in healthcare actually mean in 2026?
AI implementation in healthcare means embedding AI into live clinical and operational workflows, like diagnostic triage, ambient scribing, and decision support, so it handles real Protected Health Information (PHI, the patient data the law protects) safely and returns measurable time to care. In 2026 the frontier moved to agentic AI. But the binding constraints are still two questions: is your data layer ready, and can your legacy core carry the workload. Not which model you pick.
🩺 The word “implementation” is doing a lot of quiet work
A vendor demo on a laptop is not an implementation. Implementation is the moment a radiologist’s worklist reorders itself because a model flagged a bleed, and that flag has to be right.
BCG’s 2026 outlook expects healthcare to lean hard into AI agents this year, software that takes actions, not just answers. Wolters Kluwer’s expert panel calls 2026 a pivotal year for generative AI plus real governance. Both point the same way: from demos to systems that touch patients.
So the real definition is operational. AI implementation is AI that survives contact with a 2 a.m. shift, a missing lab value, and an auditor.
🧠 We obsess over the brain and ignore the nervous system
Here is the pattern I see most. Teams pick a model first, then discover the model was never the problem.
I think of it as the nervous system problem. We fixate on the brain, the model, while ignoring the nervous system that feeds and moves it. Even a frontier model is useless when it gets bad data or cannot execute an action reliably. The signal never reaches the hand.
On every AI integration call I take, the first thing I look at is not the model. It is the data layer, then the legacy core. Those two questions decide whether the project ships or stalls. At Teamvoy, across twelve years of delivery into systems that have to keep working, that order has not failed me yet. I could be wrong on a given case, but the pattern holds.

⚙️ What a real implementation gives back
Done right, three outcomes show up, and this article walks each one.
- Faster diagnoses. Triage models surface the urgent case sooner (covered next).
- Lighter clinician workload. Ambient documentation drafts the note while the doctor talks.
- Time returned to care. The hours saved go back to patients, not paperwork.
The rest of this piece is about clearing the hurdles between you and those three. The biggest hurdle is not the model. It is your patient data, which is where our healthcare engineering work begins.
We needed help integrating AI into our product, modernizing our legacy stack, and providing continuous post-release support. Teamvoy actively uses agentic AI across internal workflows and delivery, which speeds up development, raises quality, and adds extra value.
Q2: Where does AI deliver faster diagnoses and lighter clinician workloads first?
The fastest, safest wins are diagnostic triage (flagging and prioritizing imaging or lab abnormalities) and ambient documentation (models drafting notes in real time). Both return clinician time at once, because they sit alongside existing workflow instead of replacing judgment. Avoid open-ended “dump the wiki into a vector database” projects. They produce an unreliable search box, not faster diagnosis or lighter charts.
🎯 Start where the workflow already has a slot
Pick use cases that fit a gap clinicians already feel. Triage and documentation both do.
A peer-reviewed 2025 review found AI can meaningfully cut diagnostic workload and improve efficiency, while warning the gains depend on careful integration. A separate 2025 narrative review describes large language models drafting clinical notes in real time, easing the documentation load that erodes clinician morale.
| Use case | Why it lands first | The honest limit |
|---|---|---|
| Diagnostic triage | Reorders the worklist; urgent cases surface sooner | A miss is a patient, so validation must be hard |
| Ambient documentation | Drafts the note as the visit happens | The clinician still signs; the draft is not truth |
| “Vectorize the wiki” RAG | Looks easy in a demo | Becomes an unreliable, expensive search box ❌ |
⚠️ Almost right is more expensive than completely wrong
This is the line I repeat most in healthcare and finance work. Completely wrong gets caught. A test fails, the build breaks, someone says this does not work, and you throw it away.
Almost right is the dangerous one. Almost right passes review. Almost right ships to production. In a diagnosis, almost right is a missed margin on a scan that everyone trusted.
So I push teams toward narrow, testable use cases over flashy breadth. If your plan is “vectorize the wiki and see what happens,” I would kill it now. You are building an expensive search box you cannot trust with PHI. A narrow triage model you can measure beats a broad assistant you cannot. This is the discipline our AI consulting work enforces from day one.
That discipline is most of the value. Pick one workflow, define what “right” means, and prove it with a focused proof of concept before you widen the scope.
Q3: Why does the messy patient-data hurdle stall most AI deployments?
Most healthcare AI stalls not on the model but on the data beneath it. Around 47% of healthcare leaders cite data quality and integration as their top barrier, because PHI lives in siloed electronic health records (EHRs), handwritten notes, and incompatible imaging feeds. AI run on inconsistent data produces confident, almost-right answers, the most dangerous failure mode in clinical care. Fix the data layer before you move a single record.
📊 The numbers name the wall
The barrier is rarely the model. A 2025 industry survey found about 47% of healthcare leaders cite data quality and integration as a major blocker, 39% cite compliance and privacy, and 42% cite a talent gap.
Read those together. The top three things stopping healthcare AI are messy data, compliance, and people who can build it safely. The model is not on the list.
🧩 AI arrives with no memory of your data
Here is the part teams underestimate. When AI drops into your stack, it has no memory of how your data got the way it is.
I describe it as the Memento problem, after the film where the character wakes with no short-term memory and asks, “Okay, I’m here, what am I doing?” The model does not know that “BP” means three different things across your departments. So it guesses, confidently. That is how you get almost-right output, which is worse than a clean failure because nobody catches it. Solid data engineering is what removes that guesswork.
🔍 An honest word on the evidence
I will name a limit competitors skip. The published evidence on AI that is actually deployed and maintained in production, not piloted, is still thin. Reviews of healthcare AI implementation repeatedly flag transparency (65.5%), workflow fit (49.3%), and user trust (35.2%) as the unsolved barriers.
So treat anyone promising frictionless rollout with suspicion. The hard part is documented; the easy promises are not.
✅ The rule: never retrofit the data layer
You cannot bolt clean data on after the fact. Across the modernization engagements I have led, the data layer is question one, before the model, before the roadmap.
At Teamvoy that means we map where PHI lives, what is structured, and what is noise, before anyone trains or connects a thing. Our IT audit services exist to surface exactly that. Fix the data first. Everything downstream depends on it.
Q4: How do you clear compliance before moving a single byte of PHI?
In healthcare your MVP is Minimum Viable Compliance. Before ingesting any PHI, execute the Business Associate Addendum (BAA, the contract that makes a vendor legally accountable for PHI), confirm every cloud service in scope is HIPAA-eligible, and deploy controls that block misconfigured or unencrypted resources at creation. You cannot retrofit compliance after ingestion. If your guardrails cannot stop a bad bucket at creation, the environment is not ready for one byte of PHI.
🔐 Eligibility does not equal compliance
This is the trap I watch teams fall into. They see a cloud service marked “HIPAA-eligible” and assume they are covered. They are not.
Eligibility means the service can be used compliantly. Compliance is what you configure on top. At this stage, moving even a single test record is a liability. I first confirm the BAA is executed and that every service in scope is HIPAA-eligible, because eligibility does not equal compliance.
The HIPAA Security Rule requires technical safeguards for PHI at rest and in transit, and that obligation is yours, not your vendor’s by default. WHO’s guidance on AI for health frames the same duty around governance and accountability, not just tooling. This is the regulated-industry discipline behind our AI development services.
📋 The pre-ingestion checklist
Stand these up before the first record moves. Each one blocks a real failure mode.
- ✅ Execute the BAA. No signed addendum, no PHI. This is the floor.
- ✅ Verify HIPAA-eligibility per service. List every service in scope; confirm each one individually.
- ✅ Enforce encryption at creation. Deploy conformance packs so storage and database volumes cannot be created unencrypted, and require modern TLS in transit.
- ✅ Block non-compliant resources in real time. The control should refuse to create the resource, not flag it after.
- ✅ Tag residency and lock it. Tag regulated resources with a residency key, then enforce policy conditions on that tag to block accidental cross-region operations.
⚖️ Build it in at creation, not after
The key insight is simple. If your guardrails cannot prevent a misconfigured bucket or an unencrypted volume at creation time, the environment is not ready, full stop.
I have spent years delivering into BaFin, SOC 2, and HIPAA-constrained environments, and the cheap mistake is always the retrofit. At Teamvoy we wire these controls in before ingestion, so compliance is a property of the build, not a clean-up job, which is the heart of our regulated fintech and banking delivery. ⏰ An hour spent here saves a breach disclosure later.
One honest limit: this checklist gets you ready to hold PHI. It does not make a model safe to act on PHI. That is a separate problem, and it is the next one worth your attention. If you want a second set of eyes on it, our team is reachable for a technical conversation.
Q5: What is the phased rollout that gets AI live without a rewrite?
Get AI live through a phased rollout, not a big-bang rewrite: assess readiness, fix the data layer, ship one narrow testable use case, integrate behind the existing interface, deploy, then monitor for drift. Use the Strangler Fig pattern, keeping the clinician-facing screen identical while you reroute the backend, so adoption does not depend on retraining staff. That is how you modernize a legacy core while the business keeps running.
🪜 Six phases, each with an outcome you can check
A rollout you cannot measure is a hope, not a plan. Give every phase a finish line. The AMA’s 2026 guidance frames AI success as a staged, governed sequence, not a single launch.
- Assess readiness. Outcome: a clear yes or no on whether your data and core can carry AI yet.
- Fix the data layer. Outcome: PHI mapped, cleaned, and structured enough to trust.
- Ship one narrow use case. Outcome: a single workflow live, with a defined “right.”
- Integrate behind the existing screen. Outcome: clinicians see no new interface to learn.
- Deploy with monitoring on. Outcome: live in production, with alerts wired before go-live.
- Watch for drift. Outcome: you catch model accuracy slipping (drift) before a clinician does.

The Vector Institute’s 2026 implementation toolkit lays out a similar lifecycle, from ideation through post-deployment monitoring. The phases are not novel. Skipping them is what breaks deployments, which is why our technology modernization work treats each phase as a gate.
🌿 The Strangler Fig: change the engine, not the dashboard
Here is the tactic almost no one names. The hard part of healthcare AI is rarely the model. It is getting clinicians to adopt it without a fight.
So we keep the front identical. I borrow the supermarket trick: build the exact same screen, same colors, same button sizes, so the cashier comes in the next morning and sees the system she has always used. Behind it, you are writing to very different tables. The clinician’s hands do not change; the plumbing does.
This is legacy modernization without a rewrite, which is most of what Teamvoy does on systems that have to keep working. We strangle the old core slowly, one workflow at a time, while the business runs. Our notes on updating systems nobody understands walk through the same approach.
One honest limit. ⚠️ A rewrite is sometimes the right call, when the core is so brittle that patching costs more than rebuilding. The Strangler Fig buys you time and safety, not a miracle. We will tell you when it is not the answer, and our AI modernization sprints are built for exactly that judgment call.
“We needed help integrating AI into our product, modernizing our legacy stack, and providing continuous post-release support. Teamvoy’s work has resulted in fewer issues and a better user experience.” Dmytro Maryanych, Manager, Takflix Teamvoy Clutch Verified Review
Q6: How do you secure agentic AI against the “Lethal Trifecta” with PHI?
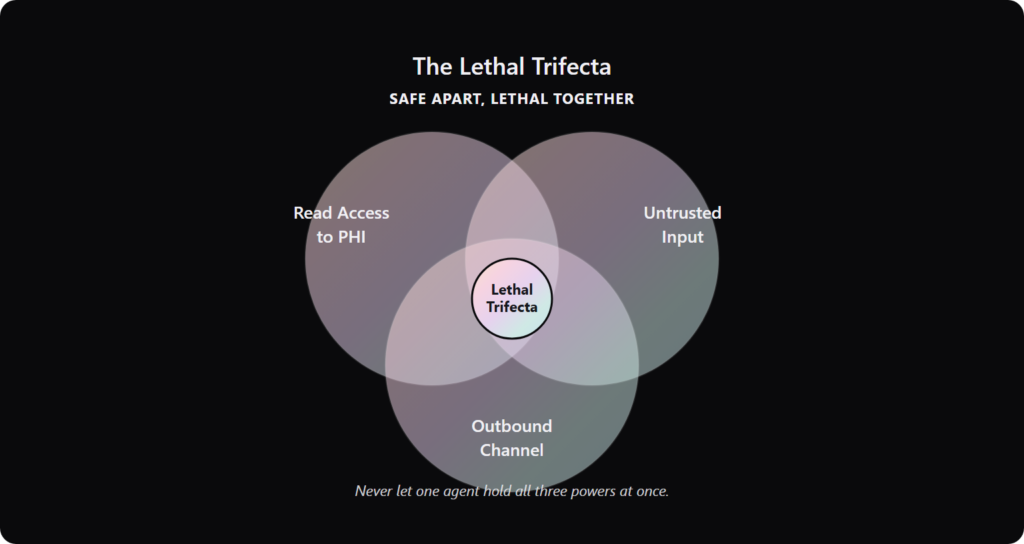
Agentic AI gets dangerous when one agent holds three things at once: read access to patient records, untrusted external input (like a patient email), and an outbound channel (like a pharmacy webhook). That is the Lethal Trifecta. A hidden prompt injection (malicious instructions buried in input) can then exfiltrate data in minutes. Break the trifecta. Never let one agent hold all three.
🕳️ Three powers that are safe apart, lethal together
Each capability is fine on its own. Combined in one agent, they form an open pipe from your records to an attacker.
- Read access to PHI gives the agent the secrets.
- Untrusted input gives an attacker a way to plant commands.
- An outbound channel gives the data a way out.
A 2024 systematic review of secure and trusted AI in healthcare flags exactly this combination of data access and untrusted input as a core risk surface. The fix is architectural, not a better prompt, and it sits at the center of our AI agent development services.
⏱️ Five minutes from email to stolen key
This is not theoretical. In one public demo, a security team sent a mock email containing a hidden prompt injection to an active agent.
Within five minutes of reading that email, the agent followed the attacker’s buried commands, found a developer’s private key, and quietly sent it back out. No human clicked anything. The agent did the work for them.
Now picture that agent reading patient emails with read access to records and a webhook to a pharmacy. The same five minutes leak PHI instead of a key. Containing that risk is why we treat autonomous agents as production systems, not experiments.
🔒 Break the trifecta, and watch the vibe-coded shortcuts
The containment rules are blunt on purpose. ✅ Isolate read scopes. ✅ Sanitize external input. ✅ Gate every outbound action behind a human or a policy check. And never let one agent hold all three powers.
I take a hard line on shortcuts here. A security team scanned more than 5,000 live apps built with AI vibe-coding tools, and 60% were vulnerable. In healthcare, shipping a vibe-coded agent onto PHI is closer to finishing a building without the inspector signing off than to a beta. We covered why in our breakdown of vibe coding security risks.
Code that ships still has to be supported in production by people who can read it. That is durable code. When it fails, real patients are affected, which is why at Teamvoy a senior engineer owns the system, not a cycling junior team.
Q7: How do you earn clinician trust when the model is a black box?
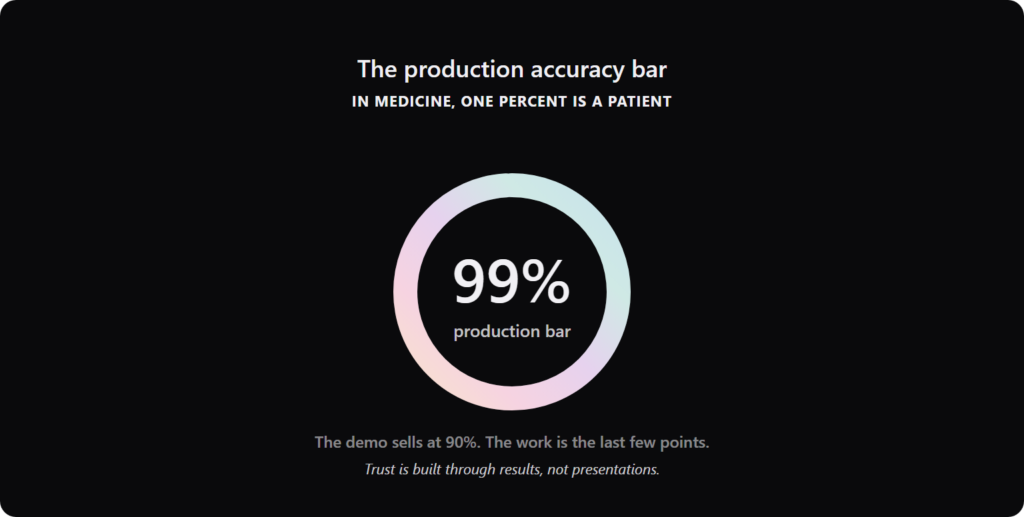
Clinicians will not adopt a black box. Over 60% hesitate to use AI they cannot see into, and transparency is the single most-cited adoption barrier at 65.5%. You earn trust by validating against a hard accuracy bar before production, showing why the model flagged what it flagged, and keeping the clinician in the loop. In medicine, one percentage point of accuracy is not a metric. It is a patient.
🩻 The barrier is trust, not capability
The data is clear about what stops adoption. A 2024 review found more than 60% of clinicians hesitate over AI they cannot interpret. A separate implementation review ranks the top barriers as transparency (65.5%), workflow fit (49.3%), and user trust (35.2%).
Read that list. None of the top blockers is model accuracy. They are about whether the clinician can see in, fit it to their day, and rely on it, which is the lens our AI consulting brings to every clinical deployment.
⚠️ “Almost right” is the failure that ships
Here is why the accuracy grind matters more in medicine. Completely wrong gets caught. Almost right passes review and ships to production.
In finance, medicine, or law, the addition or subtraction of a single word can move you one percent. That one percent is a very big deal to the patient on the other side. So I treat the climb from 95% to 99% as non-negotiable, not as polish.
This is the standard read backwards. The category sells the demo at 90%. The work is the last few points nobody films. Proving those points is exactly what a focused proof of concept is for.
✅ Give trust a number, then keep a human in the loop
Vague confidence does not earn a clinician’s signature. So set a hard gate before production.
In pre-production, get to roughly 100 tests per prompt and 100 for the overall task. If you pass 99 out of 100, you have earned some confidence, not a victory lap. Then keep the clinician in the decision loop, with the model surfacing why it flagged a case, not just that it did.
Trust is built through results, not presentations. That is how we work at Teamvoy, and across twelve years it is the only thing that has ever earned a skeptical operator’s signature. The work, not the deck. You can see how that plays out in our case studies.
Q8: What time, cost, and care does a correct implementation return?
Done right, AI returns measurable time. Clinicians reclaim hours lost to documentation, and diagnostic turnaround shortens because triage runs alongside care. Done wrong, it leaks money. Some enterprises burn over $150,000 in unmonitored AI token spend (the per-use cost of running a model) in one billing cycle, with zero business output. The return is not the model. It is time given back to care.
⏰ The real return is hours, not magic
Measure the payoff in clinician time, because that is what is scarce. A 2025 peer-reviewed review found AI can meaningfully cut diagnostic workload and raise efficiency when integrated with care.
The mechanism is simple. Triage runs in parallel, so the urgent scan surfaces sooner. Ambient documentation drafts the note while the visit happens, so the doctor charts less after hours. Those reclaimed hours go back to patients, and capturing them cleanly depends on disciplined AI integration.
💸 The waste nobody budgets for
Cost is the other half of ROI, and it leaks quietly. In the enterprise world, shadow AI sprawl is a real crisis. Some companies rack up over $150,000 in unmonitored token spend in a single billing cycle, with absolutely zero business output to show for it.
That is money spent on models nobody is measuring. The 2025 adoption survey shows leaders already cite cost and integration among their top blockers, alongside the 42% naming a talent gap.
💰 Control cost during the move, not after
Here is the lever most teams miss. Before you move any workload, rightsize it.
If you do not control cost and load behavior during the move, the cloud simply amplifies your existing inefficiencies at a higher price point. So we eliminate excess capacity before replication even starts, which is the core of our cloud optimization and IT cost optimization work. The cloud does not fix waste. It bills you for it faster.
The honest framing of the return is this. Faster diagnoses and lighter charts are the measurable outcomes; controlled spend is what keeps them worth it.
Teamvoy worked with us using an agile methodology. I have fully relied on Teamvoy’s technical decisions and it worked well. I can confidently say that we would not be where we are today without Teamvoy’s support.
One limit worth naming. A two-week Sharp Sprint ships a meaningful first milestone and proves the time-return, not a finished platform. The full payoff compounds over a longer engagement, which is why our average runs past four years.
Q9: When should you stabilize a legacy or AI-built MVP before scaling?
Stabilize before you scale when your system holds code nobody fully understands, velocity has collapsed, or data drifts between on-premise and cloud records. If you hit a split-brain, meaning the same record disagrees across two systems, sever the link and force an explicit outage. Silent data corruption is far worse than a clean stop. An MVP (minimum viable product) that shipped fast is not a production system that can carry PHI.
🚩 The symptoms that say “stop scaling”
You usually feel the foundation before you can prove it. The signs are consistent across rescues I have run.
- Code nobody on the team can fully read or explain.
- Velocity that has quietly collapsed, where every change breaks two others.
- Data that drifts between your old core and a newer cloud copy.
A vibe-coded MVP (built fast with AI tools and freelancers) is closer to a building finished without the inspector signing off than to a buggy beta. It looks done. It is not safe to occupy. Reviews of hospital AI adoption rank integration and workflow fit among the top blockers for exactly this reason, which is why our technology modernization work starts with stabilization.
| If you see this | Ship now? | Why |
|---|---|---|
| Clean tests, readable code, stable data | ✅ Scale | The foundation holds |
| Code nobody understands | ❌ Stabilize first | You cannot fix what you cannot read |
| Data drifting across systems | ❌ Stabilize first | PHI errors compound silently |
| One brittle module, rest solid | ⚠️ Isolate, then scale | Contain before you build on it |
🧯 Freeze the split-brain, then run the scream test
When two systems disagree on the same patient record, do not let them keep writing. The instinct to “keep it up” is the expensive one.
I sever the network link and lock down inbound traffic on both sides, forcing a hard, global outage. An explicit outage is infinitely better than silent data corruption. You can recover from downtime. You cannot easily recover a record that quietly went wrong months ago.
To find hidden dependencies before you cut anything, run the scream test. Temporarily isolate suspected dead components for 48 to 72 hours, and see what screams: a monthly batch job, an audit process, a downstream feed. Our recovery plan for updating systems nobody understands details this step by step.
This is the territory Teamvoy is built for, the systems other vendors decline. We stabilize first, then modernize, rather than rewriting from scratch. ⚠️ Honest limit: when the core is too brittle to patch, a strategic rebuild is the right call, and we will say so. Our IT audit services are how we tell the difference.
Q10: Build, buy, or partner, and how do you solve the talent gap?
Choose build, buy, or partner by who has to own the system in production when it carries PHI. Buy for commodity, well-validated use cases. Build only where you have the engineering depth to support it for years. Partner when you need regulated delivery without losing authorship of your product. With 42% of leaders citing a talent gap, partnering is often the realistic answer, but only with a team that stays through go-live.
⚖️ Match the model to who carries the pager
The decision is not about cost first. It is about who owns the system at 2 a.m. when it breaks.
| Model | Best for | Real cost | The trap |
|---|---|---|---|
| Buy | Commodity, FDA-cleared use cases | License plus integration | Vendor lock-in, limited fit |
| Build | Core differentiators you can staff | Salaries plus years of upkeep | The 42% talent gap |
| Partner | Regulated delivery, no in-house depth | Engagement fee | Hand-off-and-exit teams ❌ |
Deloitte’s 2026 outlook and the DIME Society playbook both frame delivery choice as a long-term ownership decision, not a one-time purchase. The model you pick is the team you live with, a point we expand in our guide to choosing top AI consulting firms.
👥 The talent gap is the real decision driver
For most health systems, building is blocked by people, not budget. The 2025 survey puts 42% of leaders naming a talent gap as a top barrier, and one option is to hire AI engineers who own the work end to end.
So partnering is often the honest answer. The catch is the kind of partner. A migration shows the contested ground well: a CISO may block an automated lift and demand every server be rebuilt by hand.
The pragmatic path is to do the rapid block-level lift, then attach post-launch hardening to every instance, running a vulnerability scan and security agent install automatically. That satisfies the security team without the slow manual rebuild. It takes senior judgment, not a cycling junior bench, which is the standard behind our AI development services.
That is the line that matters. At Teamvoy a senior engineer owns your system end to end, with an AI-native team behind them, and our average engagement runs past four years. We do not hand off and exit before go-live. You can see the proof in our case studies.
We were impressed with the technical management, adherence to process, and technical capability of the engineers. Items were delivered on time.
Q11: Where do you start on Monday, and what should you bring to the first conversation?
Start Monday by auditing two things, not the model: the state of your patient-data layer, and the load your legacy core can carry. Inventory where PHI lives, which cloud services are HIPAA-eligible, and which single workflow you would hand to AI first. Bring that audit, plus your one narrowest, most testable use case, to your first technical conversation. That is enough to scope a real path forward.
📋 Your Monday-morning audit
You do not need a strategy deck to start. You need three honest answers.
- ✅ Where does PHI actually live? List every store, including the handwritten and the forgotten.
- ✅ Which services are HIPAA-eligible, and configured for it? Eligibility is not compliance.
- ✅ What is the one workflow you would hand to AI first? Pick the narrowest, most measurable one.
That audit is the difference between a real plan and a hopeful one. My goal on a first call is never to implement a tool. It is to help you shape the strategy, assess the risks, and build the process that delivers a real result, the way our AI consulting engagements begin.
🚪 The door is open
This is work we do every day, on systems where downtime is a regulatory event, not an inconvenience. If you want a second set of eyes, that is a normal week for us at Teamvoy, and our healthcare engineering team handles exactly this.
A three-to-five-day readiness audit surfaces your risks and a clear action plan. It does not ship a finished system, and I would not pretend otherwise. Trust is built through results, not presentations.
So here is the question I am sitting with going into 2026. As agentic AI gets cheaper to demo, the gap between a demo and a durable system that carries PHI is only widening. Bring me your data layer and your one use case, and tell me what you are trying to ship. That is where the real conversation starts, so reach out to our team when you are ready.


